
Hemophilia is usually inherited. The hemophilia gene is passed down from parent to child.
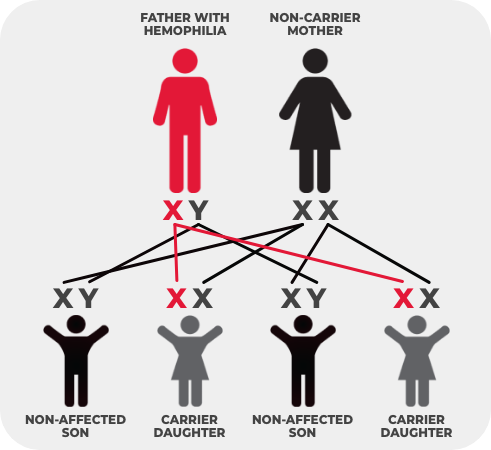
When the father has hemophilia, but the mother does not, none of the sons will have hemophilia. All of the daughters will carry the hemophilia gene.
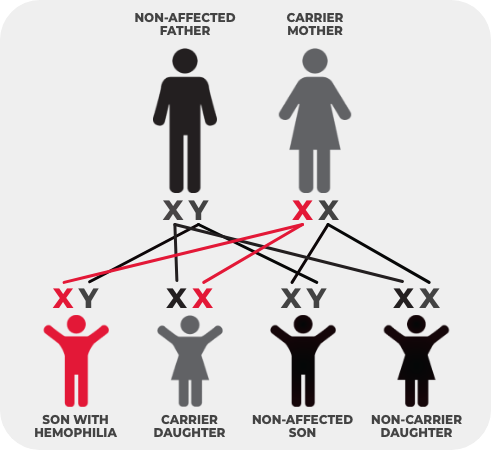
If a woman inherits a copy of the altered gene from either of her parents, she is said to “carry” the hemophilia gene and is therefore called a “carrier.” In other words, she has one normal and one altered copy of the gene.
- She can pass either gene on to her children.
- For each child, there is a 50% chance that a son will have hemophilia and a 50% chance that a daughter will carry the gene.
Factor Levels in Carriers
Hemophilia A is characterized by a lack of factor VIII clotting protein in the blood that results in prolonged bleeding.
Most female carriers have normal factor VIII levels and do not experience any abnormal bleeding. However, some women have low factor VIII levels, similar to men with mild hemophilia A, and experience excessive, prolonged, heavy, or abnormal bleeding at times of menstruation, childbirth, injury, or surgery.
Potential Bleeding Symptoms for Hemophilia A Carriers
| Symptom | Description |
|---|---|
| Easy bruising | Bruises are considered significant when there are 5 or more (>1 cm) in an exposed area, petechiae (small red or purple spots caused by bleeding into the skin), or hematomas (a solid swelling of clotted blood within the tissues) when occurring without trauma. |
| Nosebleeds | Any nosebleed, especially occurring after puberty, that causes patient concern (e.g., interference or distress with daily or social activities) is considered significant. It should not be considered significant when it lasts less than 10 minutes. |
| Prolonged bleeding from minor wounds | Any bleeding episode caused by superficial cuts (e.g., by shaving razor, knife, or scissors) or that requires frequent bandage changes is considered significant. Insignificant bleeding from wounds includes those lasting less than 10 minutes and lesions that usually require stitches in those without hemophilia (e.g., under the chin). |
| Prolonged bleeding after surgery or invasive procedures | Prolonged or heavy bleeding may occur following surgery or any type of an invasive procedure (e.g., tooth extraction, dental cleaning, colonoscopy, or endoscopy). Inhibitor testing is advised prior to the surgery or invasive prodecure. |
| Heavy menstrual bleeding |
Heavy menstrual bleeding, or menorrhagia, is the most common bleeding symptom experienced by hemophilia A carriers or women with mild hemophilia A. Women with lower factor VIII levels are at greater risk for excessive blood loss during the menstrual period. Signs of abnormal menstrual bleeding:
|
| Heavy bleeding after childbirth | Heavy bleeding after childbirth can occur anywhere from 24 hours to 6 weeks following delivery. Hemophilia A carriers are at risk of delayed bleeding up to 35 days postpartum. Therefore, it is important that they are seen by their physician 2 weeks postpartum and then followed-up for approximately 1-2 months to monitor postpartum bleeding. |
Easy bruising
Bruises are considered significant when there are 5 or more (>1 cm) in an exposed area, petechiae (small red or purple spots caused by bleeding into the skin), or hematomas (a solid swelling of clotted blood within the tissues) when occurring without trauma.
Nosebleeds
Heavy bleeding after childbirth can occur anywhere from 24 hours to 6 weeks following delivery. Hemophilia A carriers are at risk of delayed bleeding up to 35 days postpartum. Therefore, it is important that they are seen by their physician 2 weeks postpartum and then followed-up for approximately 1-2 months to monitor postpartum bleeding.
Prolonged bleeding from minor wounds
Any bleeding episode caused by superficial cuts (e.g., by shaving razor, knife, or scissors) or that requires frequent bandage changes is considered significant. Insignificant bleeding from wounds includes those lasting less than 10 minutes and lesions that usually require stitches in those without hemophilia (e.g., under the chin).
Prolonged bleeding after surgery or invasive procedures
Prolonged or heavy bleeding may occur following surgery or any type of an invasive procedure (e.g., tooth extraction, dental cleaning, colonoscopy, or endoscopy). Inhibitor testing is advised prior to the surgery or invasive prodecure.
Heavy menstrual bleeding
Heavy menstrual bleeding, or menorrhagia, is the most common bleeding symptom experienced by hemophilia A carriers or women with mild hemophilia A. Women with lower factor VIII levels are at greater risk for excessive blood loss during the menstrual period.
Signs of abnormal menstrual bleeding:
- Consistent bleeding for more than 7 days each month
- Pads/tampons are heavily saturated and changed every 1‑2 hours
- Use of double sanitary protection (wearing pads and tampons)
- Daily activities are impacted due to bleeding or fatigue (e.g., school, work, or social activities)
- More than 80 mL of blood loss with menstrual flow
- Sanitary protection must be changed during the night
- Symptoms of anemia, such as tiredness, fatigue, or shortness of breath
Heavy bleeding after childbirth
Heavy bleeding after childbirth can occur anywhere from 24 hours to 6 weeks following delivery. Hemophilia A carriers are at risk of delayed bleeding up to 35 days postpartum. Therefore, it is important that they are seen by their physician 2 weeks postpartum and then followed-up for approximately 1-2 months to monitor postpartum bleeding.
Pregnancy
For carriers, factor VIII levels can increase during pregnancy. Therefore, it is recommended to have levels checked in the third trimester to assess bleeding risk at the time of birth and in the postpartum period. Factor replacement therapy, if required, should be administered to maintain factor levels above 50 IU/dL for labour and delivery, and maintained in the normal range for at least 3 days after vaginal delivery or at least 5 days after caesarean delivery.

Within 1-2 weeks of delivery, factor VIII levels will fall rapidly back to baseline levels. It is important to monitor and maintain factor levels post-delivery as carriers are at increased risk of postpartum hemorrhage. Contact your hematologist if blood flow increases or large blood clots are passed.
Hemophilia A Carrier Testing
Girls or women who have a family history of hemophilia A have a chance of being a carrier of the factor VIII genetic mutation.
- Blood work is often the first step to determine if your factor VIII levels are low. Some women may not discover they have hemophilia A, or are a carrier, until later in life after experiencing prolonged or excessive bleeding following a surgery, trauma, or childbirth.
- Genetic testing is another way to confirm carrier status since hemophilia A carriers’ factor VIII levels may fall within normal range.
Psychosocial Support
- Carriers may require referral to psychosocial professionals (e.g., psychologists) for further support to address psychological or emotional issues that may arise during the genetic counselling process or at different life stages.
- Collaboration between psychosocial professionals and genetic counsellors can enhance overall patient care.
- Carriers may experience a wide range of emotional and psychosocial impacts, including feelings of guilt, sorrow, and self-blame related to reproductive choices or consequences such as passing on their genetic variant.
- It is important for hemophilia treatment centres and healthcare providers (especially genetic counsellors and clinical geneticists), families, and patient organizations to be aware that the experience of being a hemophilia carrier may change with different life stages, and carriers may need genetic and/or psychosocial counselling more than once during their lifetime.
About the Author
